Medical Journal
Published by
Faculty of Medical Sciences,
University of Sri Jayewardenepura,
Nugegoda,
Sri Lanka.
Original Articles
Knowledge and attitudes on postpartum depression among family members attending antenatal clinical in Ratnapura and Colombo districts.
Mirshan S1*, Wanigasooriya P A1, Ranasinghe R C1, Gunawardana I N1, Wickramaarachchi I U1, Shiyam A2, Seneviwickrama K L M D2, Seneviratne Alles S M P3
1Faculty of Medical Sciences, University of Sri Jayewardenepura
2Department of Community Medicine, Faculty of Medical Sciences, University of Sri Jayewardenepura
3Department of Psychiatry, Faculty of Medical Sciences, University of Sri Jayewardenepura
*me93709@sjp.ac.lk
Abstract
Background: Postpartum depression (PPD) is a complex mix of physical, emotional and behavioural changes that occur in postpartum mothers within the first 2-4 weeks of childbirth. It has a global prevalence of 17.22% which originate in the latter part of the pregnancy. A sound knowledge among the close family members is detrimental to avoid negligence and provide the necessary care for PPD.
Objectives: To describe knowledge and attitudes regarding PPD and factors associated among family members of pregnant women attending antenatal clinics in selected Medical Officers of Health (MOH) areas in Ratnapura and Colombo districts.
Methods: A descriptive cross-sectional study was conducted among 216 immediate family members in the aforementioned settings selected through multi- stage sampling using a validated, pretested, interviewer administered questionnaire. Knowledge and attitude were dichotomized using mean scores of the pilot test (knowledge 67% and attitudes 65%). Data analysis was done using SPSS version 25 and associations were determined with chi-square test using p<0.05 as the level of significance.
Results: Response rate was 97.7% (n=211), among them 68.7% (n=145) were males. Majority, 61.6% (n=130) had a good knowledge (mean score-19.23, mean percentage-68.7%) and positive attitudes 64.9% (n=137) (mean score-34.53, mean percentage 69.1%) towards PPD. Knowledge was significantly higher among those with positive attitudes (p=0.0001) and those who have seen a mother with PPD (p=0.0001). Association between knowledge and religion was statistically significant (p=0.039), but other factors were not.
Conclusion: Good knowledge and positive attitudes prevailed among most of the family members regarding PPD, despite the existence of some gaps in knowledge.
Introduction
Postpartum Depression (PPD) is a mental health problem commonly found amongst postpartum females. Its prevalence has been reported both nationally and internationally. If PPD is left untreated, it can interfere with mother- child bonding & cause issues within family. For mothers, it can last long & become chronic depressive disorder and even result in suicide, therefore women need early detection and appropriate care.
PPD usually occurs within 4 weeks after delivery of the baby (1). Apparently, most postpartum women develop depression while staying at home, under the care of their husbands and other relatives (2). Therefore, husband and relatives possibly play an important role and should be able to take care of postpartum mothers during this critical period.
Although there is research that are being carried out worldwide in order to identify the risk factors, causes and preventive measures for postpartum depression, the number of research that focuses on the knowledge and attitudes among family members are very scarce. And in Sri Lanka, there hasn’t been any proper research done so far in this topic. So, there is also a need to do this research in order to find out the knowledge gaps which exist between our people compared to other countries.
Our objective of the research is to assess the knowledge, attitudes of family members towards postpartum depression and their associated factors. In this way, we’ll be able to identify the need for awareness among people regarding this. In Sri Lanka, EPDS is usually done when the new mothers visit the clinics at the end of 1 month after delivery, so there is a period of a month where the possibilities of developing PPD are high without proper surveillance. By doing this research we are trying to assess the awareness on PPD among family members which can be used as a guide to educate them in order to promote the wellbeing of women after delivery.
Methodology
A descriptive cross-sectional study was carried out among immediate family members accompanying pregnant women in the antenatal clinics in Ratnapura divisional council Medical Officer of Health (MOH) area in Ratnapura district, Homagama MOH area in Colombo district. Family members of the pregnant women attending antenatal clinics were selected using the multistage sampling technique and those who were less than 18 years of age were excluded from the study.
The study instrument was an interviewer- administered questionnaire adapted from the researches “Knowledge and attitudes of family members towards postpartum depression” (3), “Knowledge and attitudes about postpartum depression in the Portuguese general population” (4) and “Community awareness on postpartum depression (5). Certain sections from the questionnaires of these researches were taken to form the study instrument for data collection and some modifications were done with the consent of the authors. The modified questionnaire was given for content validity to the experts of the field and then it was finalized incorporating the suggestions given by them. Prior to proper data collection, the questionnaire was pretested.
The questionnaire consisted of 3 sections: Sociodemographic information, knowledge on postpartum depression, attitudes regarding postpartum depression.
For the assessment of knowledge marks were allocated in two ways; For the questions which tested the knowledge.
Correct answer 1
Wrong answer/ Don’t know 0
Tables which tested the knowledge on causes and symptoms were marked using the YNDK scale.
Yes 2
No 0
Don’t Know 1
Marks for the causes and symptoms were given out of 30 and 40 respectively and expressed out of 10. The total scores for the knowledge portion were calculated as a percentage out of 28. According to the mean score of the pilot test anyone with a score greater than 67% was considered to have good knowledge.
Attitudes were assessed according to the Likert scale. There were 25 statements in total regarding the attitudes towards Postpartum depression and the following marks were given,
Strongly agree/ Agree 2
Neutral 1
Strongly Disagree/ Disagree 0
The total marks for the attitude section were calculated as a percentage out of 50 (2*25).
According to the mean score of the pilot test, if the marks exceed 65% the person is considered to have ‘positive’ attitudes towards postpartum depression and if he/she scores less than 65% the person is considered to have negative attitudes.
Data analysis was done using Statistical Package for Social Sciences (SPSS) program (version 25). The ethical clearance was obtained from the Ethics Review Committee of Faculty of Medical Sciences, University of Sri Jayewardenepura prior to any data collection.
Results
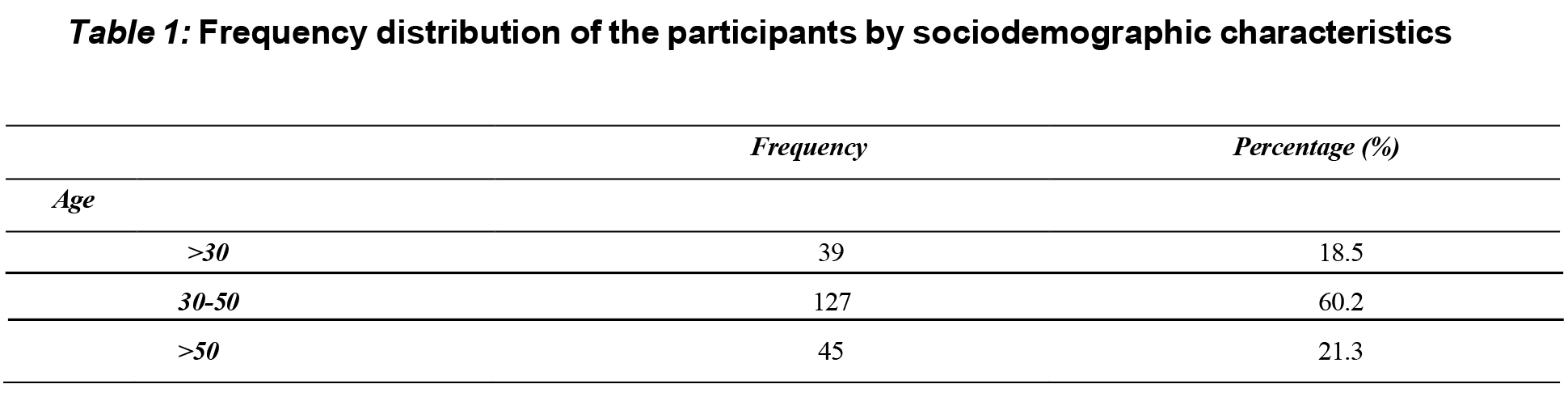
According to table 1, majority of the respondents were husbands of the pregnant women (n=135, 64%), Buddhists n=195 (92.4%). The bulk of the participants were married n=197 (93.4%). All the participants have had school education n=211 (100%).
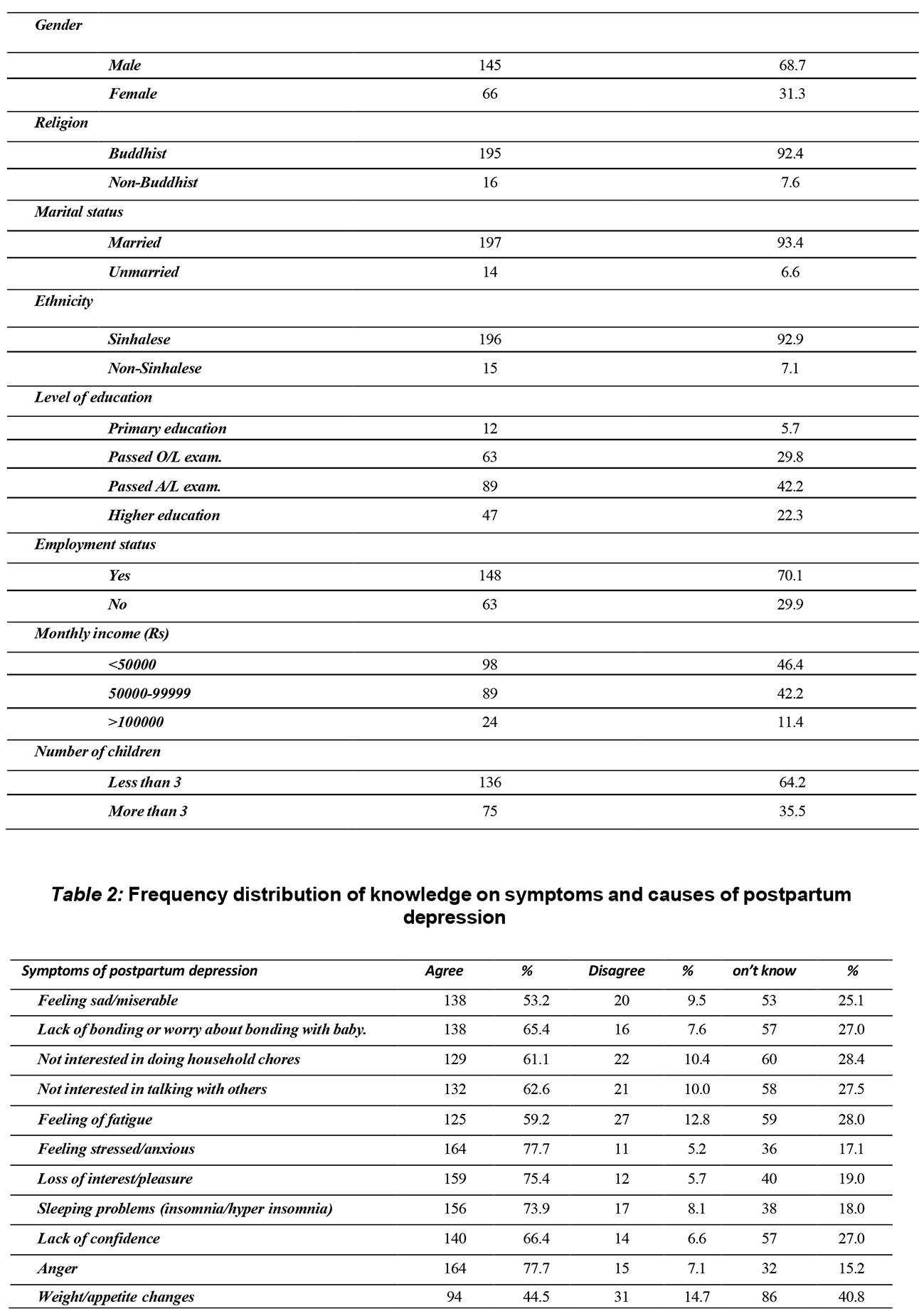
According to table 2, only 139 respondents (65.9%) knew the exact term postpartum depression while 72 respondents (34.15%) were unaware of the exact term although they knew about postpartum depression. Internet/media ranked the highest 38.8% (n = 139) as the initial source of information from all the sources that were provided (mass media, social media, school/university, family/friends, other). Most of the interviewees had not seen a mother with postpartum depression before (n=164, 77.7%) and only 26 respondents (12.3 %) had heard of the Edinburgh postnatal depression scale.
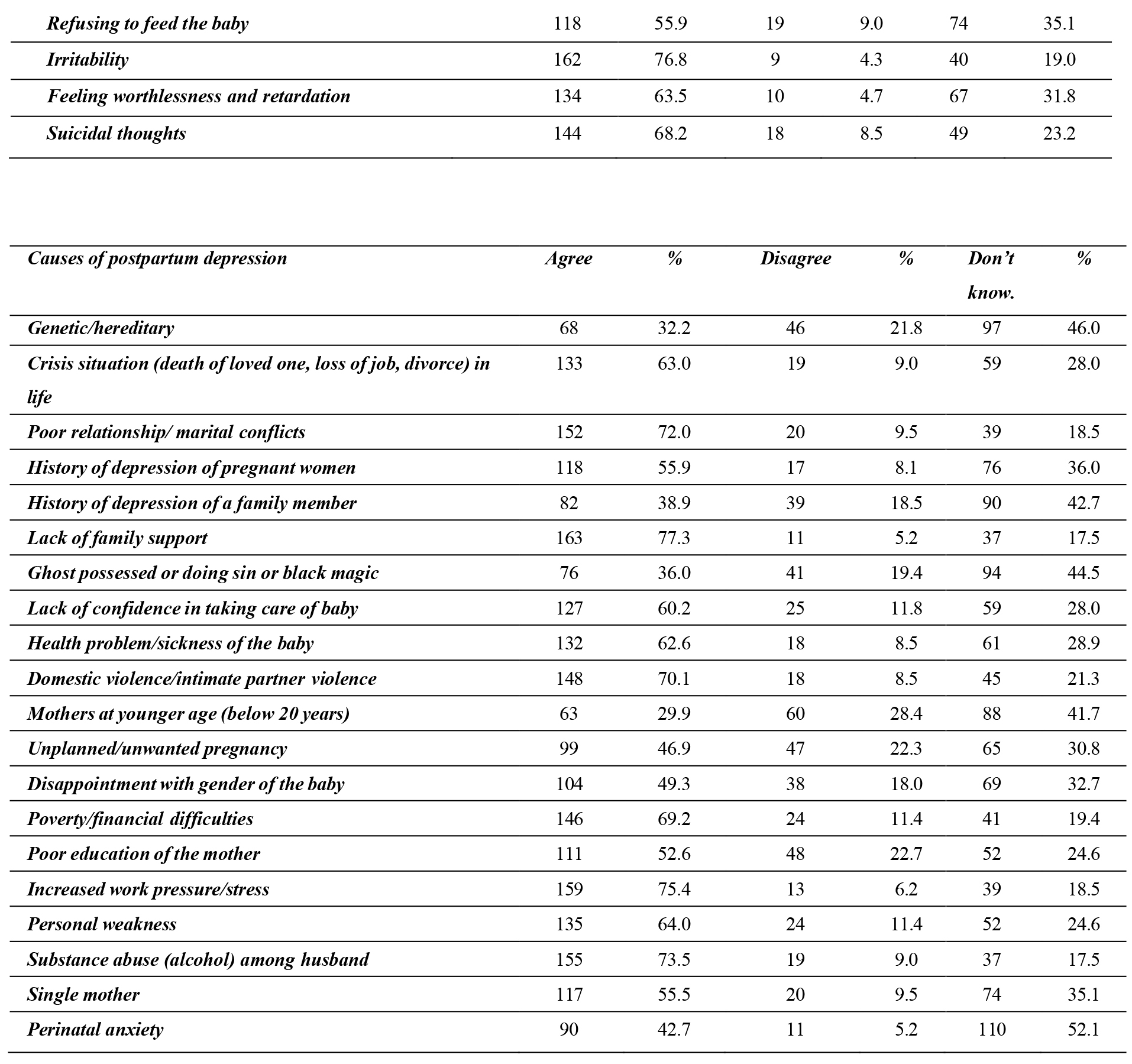
Majority of participants identified the symptoms of postpartum depression such as anger (77.7%), feeling stressed/anxious (77.7%), loss of interest/pleasure (75.4%) while they failed to identify weight/appetite changes (44.5%) as symptom of PPD. Concerning the causes of postpartum depression, most of the participants accorded to the given causes except unplanned/unwanted pregnancy (30.8%), disappointment with gender of the baby (32.7%), history of depression of pregnant women (36.0%), single mother (35.1%), which were not known by the most of respondents. And at the same time a significant number of participants disregarded genetic/hereditary and mother at younger age as a cause for postpartum depression.
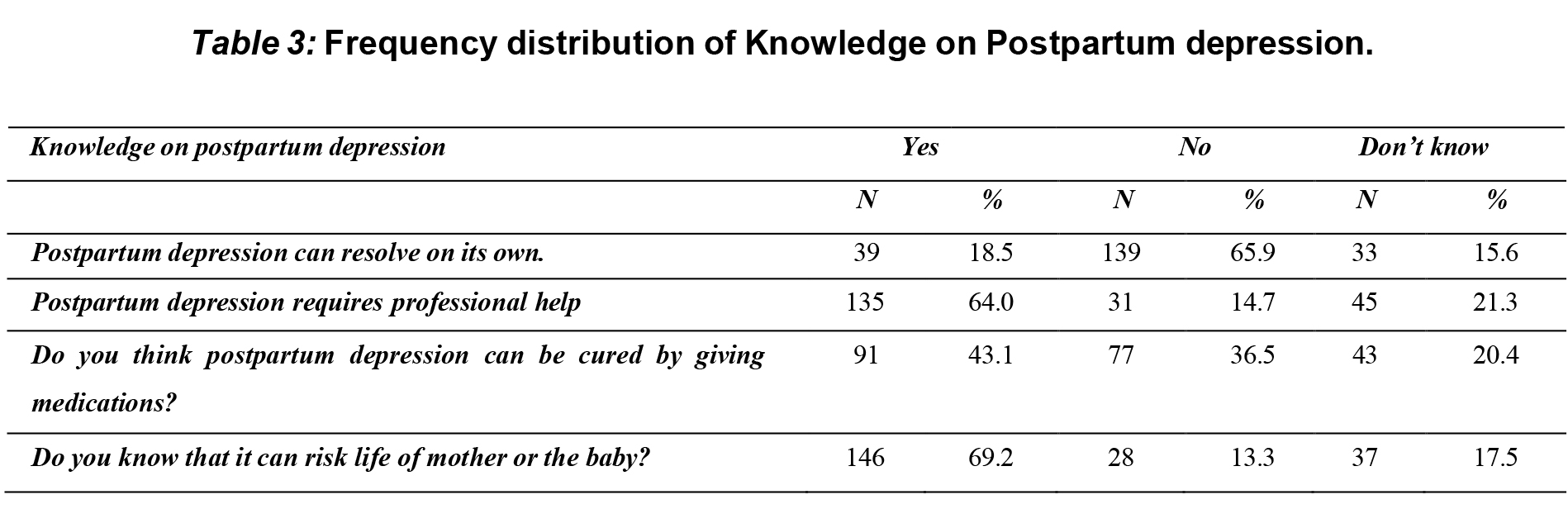
According to table 3, most of the participants (65.9%) had responded as postpartum depression cannot resolve on its own and had said that postpartum depression requires professional help (64.0%), and they know that it can risk the life of mother or the baby (69.2%).
Although most respondents think that postpartum depression can be cured by giving medications (43.1%), nearly equal amount had said it cannot happen that way (36.5%).
Based on the mean value obtained from the pilot test (67%), the participants were categorised as good and poor for the knowledge on postpartum depression.
A large number of interviewees had good knowledge on postpartum depression (n = 130, 61.6%), whereas only 81 respondents (38.4%) had poor knowledge levels regarding postpartum depression.
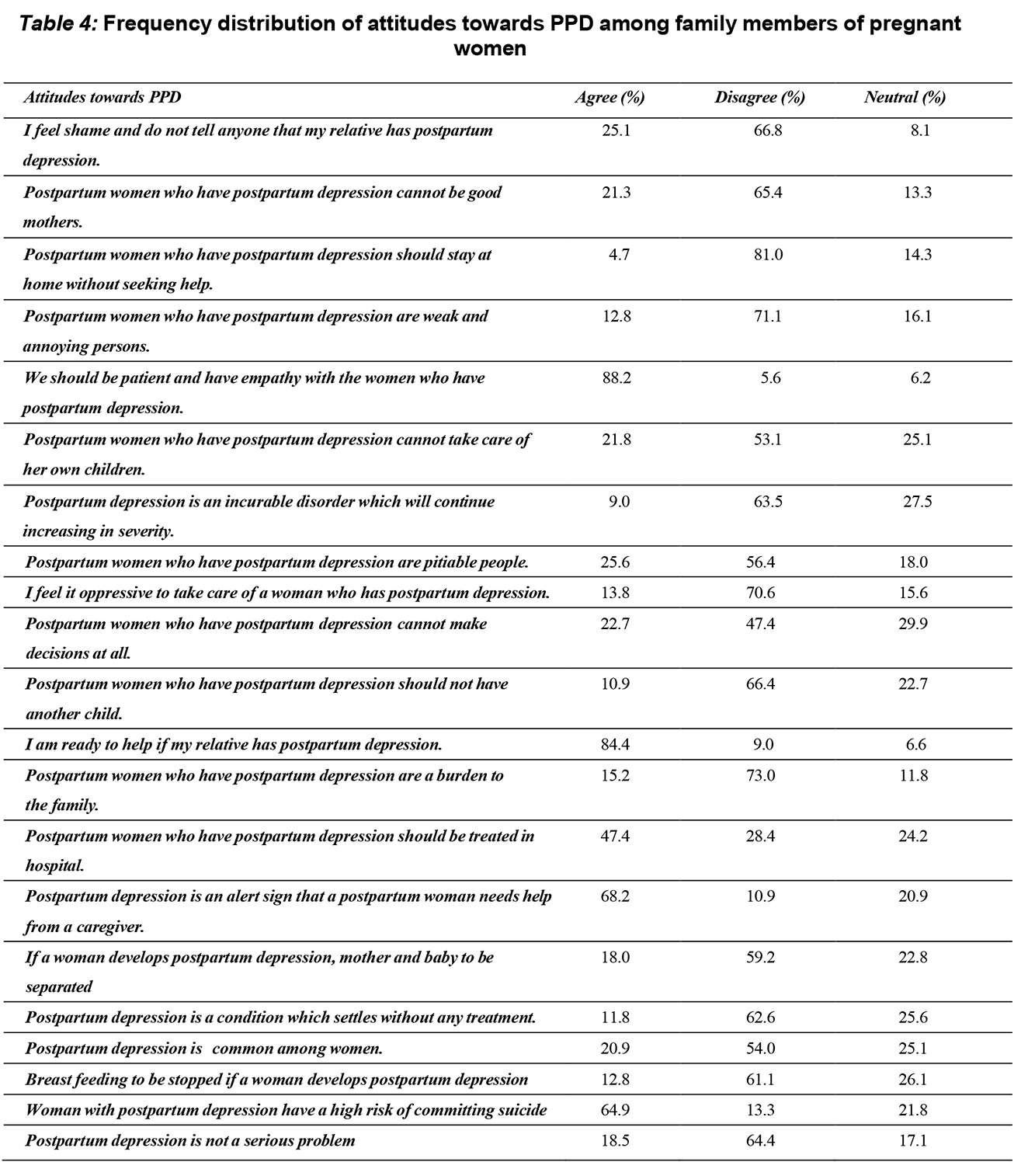
According to table 4, a majority of participants agreed that they should be patient and have empathy with the women who have postpartum depression (88.2%), they are ready to help if their relative has postpartum depression (84.4%), and postpartum depression is an alert sign that a postpartum woman needs help from a caregiver (68.2%).At the same time majority of the respondents had disagreed that the postpartum women who have postpartum depression should stay at home without seeking help (81.0%), postpartum women who have postpartum
depression are weak and annoying persons (71.1%), they feel it oppressive to take care of a woman who has postpartum depression (70.6%), postpartum women who have postpartum depression are a burden to the family (73.0%).
Based on the mean (65.0%) obtained from the pilot test, the participants were categorised as having good and poor attitudes towards the postpartum depression. The majority of interviewees (n =137, 64.9%) hold positive attitudes, while (n=74, 35.1%) of the respondents had negative attitudes.

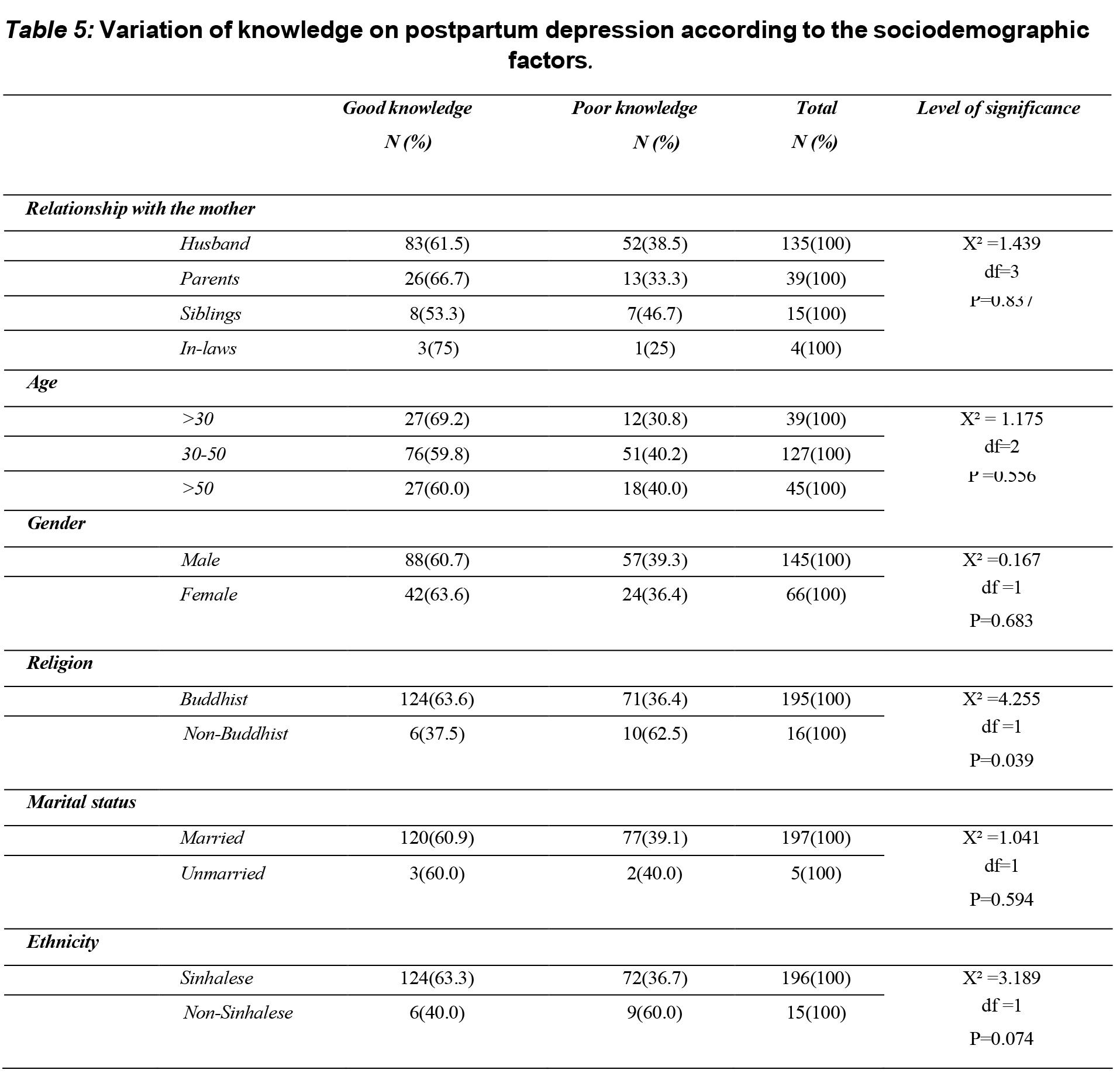
According to table 5, 63.6% of Buddhist women have good knowledge on PPD. But among non-Buddhist participants only 37.5% have good knowledge on PPD. A significant difference can be observed statistically. (p =0.039).
There is no statistically significant association between the factors of employment status (p=0.574), number of children (p=0.343), age (0.556), educational level (p=0.779) and the knowledge on PPD.
Among participants who have ever seen a mother with PPD, majority (n=42, 89.4%) had good knowledge on postpartum depression, while among the population who have never seen a mother with PPD, majority (n=88, 53.7%) had good knowledge on postpartum depression. This observed difference was statistically significant (p<0.0001).
There is no statistically significant association between the factors, relationship with mother(p=0.488), age(p=0.961), sex(p=0.564), religion(p=0.193), Ethnicity(p=0.329), employment status(p=0.976), educational level (p= 0.052), the no. of children (0.514), alcohol consuming (p =0.146), smoking (p=0.286) and attitudes towards PPD.
Among participants with good knowledge on PPD, majority (n=101, 77.2%) expressed good attitudes towards PPD, while among the population with poor knowledge, 44.4% expressed good attitudes towards PPD. This observed difference was statistically significant (p<0.0001).
Discussion
A large proportion of participants in our study had good knowledge and positive attitudes regarding postpartum depression which was congruent to the findings by other studies (3,4,6), despite the existence of some gaps in knowledge and some stereotypes. The results were as expected, out of the participants 61.6% had good Knowledge on PPD and 64.9% of the participants had positive attitudes towards PPD.
Most participants even though they knew the time period in which postpartum depression is developed, they weren’t aware that a tool like Edinburgh postnatal scale was available to assess postpartum depression. Most participants identified the symptoms of postpartum depression such as anger (77.7%), feeling stressed/anxious (77.7%), loss of interest/pleasure (75.4%), which match the findings of Sealy et al., (2009) and Poreddi et al., (2020).
Concerning the participants attitudes towards postpartum depression most of them denied the fact that women with PPD are weak and annoying people (71.1%), a woman with postpartum depression is a burden to the family (73.0%). Furthermore, they agreed to help women with PPD, to be patient with them and to show empathy towards them. Although the results coincide with results of study done in India, the results of that research showed that they feel ashamed to reveal the fact that they have a patient with PPD in their family (3). We assume that this is due to the difference in cultural beliefs between the two countries.
Association between Attitudes, knowledge and sociodemographic factors ……..
Numerous studies have suggested that poorly educated people may have had minimal learning opportunities with regard to mental health problems in general and about PPD specifically, which would result in sub-par level of knowledge and more negative attitudes towards PPD (7,8). Our study failed to show a significant association between factors such as the educational qualification, age with knowledge and attitudes of the participants. The lack of significant association between age with knowledge and attitudes may be due to the fact that most participants from our research belonging to the 30-50 age category rather than extremes of age. Study done in Portugal had assessed the association between the people who had personal or distant contact or experience with postpartum depression and their knowledge and attitudes (4). Although approximately half of the sample did not have personal or distant contact, the ones who did, have good knowledge and positive attitudes towards PPD which was also similar to the results of our study.
High chances of noticing gender differences in knowledge and attitudes about PPD may occur because PPD is mostly associated with female sex, and thus women may feel a great need to become and thus women may feel a great need to become informed about PPD characteristics to be able to identify and recognize it and get treatment for it and at the same time treat the same sex in a better way. However, gender or sex did not emerge as significant predictors of knowledge (p=0.683) and attitudes (p=0.564). Most of the other similar research had predominantly female participants as women attending clinics were mostly accompanied by their mothers or sisters. But our study had more male participants most probably due to the ongoing economic and fuel crisis situation in the country. People were required to work from home and due to transport issues mothers were mostly accompanied by their husbands which could be the main reason for our study having more male participants compared to other studies.
In a country where there is free education for all disregarding any difference in religion or ethnicity, it is expected to have near equal knowledge and attitudes regarding PPD in our community. Our study showed that there was no significant relationship between religion and ethnicity with attitudes. However, a significant association was noticed between the knowledge regarding PPD and the religion of the participants where the majority (Buddhists) had good knowledge over the minority. But at the same time there was no significant association between ethnicity and the knowledge level of the participants. The difference may have arisen due to the fact that the number of non- Buddhist participants were low and the value indicated might not be indicative of the collective knowledge of the rest of the community, rather just an indicator of the small quantity of people who participated in the study resulting in a lack of generalizability.
Limitations
Sri Lanka is a country which has majority of its population as Sinhalese (74.9%) while the rest (25.1%) constitutes of Tamils, Malays, Moors, Burghers, Muslims and so on according to the 2012 census (9). Most of the people who participated in the study belonged to the majority Sinhalese (92.9%) while the non-Sinhalese respondent only constituted 7.1%. Hence, the results do not exactly represent the general population of the country as the minority communities are underrepresented in our sample. The sample size had to be minimized with the COVID outbreak as an interview administered questionnaire was used as the data collection tool.
Conflicts of interests
Authors declare that there are no conflicts of interest.
Acknowledgment
Department of Community Medicine, Faculty of Medical Sciences, University of Sri Jayewardenepura.
References
- Andrews-Fike A review of postpartum depression. Prim Care Companion J Clin Psychiatry. 1999;1(1):9–14.
- Jorm AF, Barney LJ, Christensen H, Highet NJ, Kelly CM, Kitchener BA. Research on Mental Health Literacy: What we know and what we Still Need to know. Aust New Zeal J Psychiatry. 2006;40(1):3–5.
- Poreddi V, Thomas B, Paulose B, Jose B, Daniel BM, Somagattu SNR, et al. Knowledge and attitudes of family members towards postpartum depression. Arch Psychiatr Nurs [Internet]. 2020;34(6):492–6. Available from: https://doi.org/10.1016/j.apnu.2020.09.003
- Branquinho M, Canavarro MC, Fonseca A. Knowledge and attitudes about postpartum depression in the Portuguese general Midwifery [Internet]. 2019;77:86–94. Available from: https://doi.org/10.1016/j.midw.2019.06.016
- Sealy PA, Fraser J, Simpson JP, Evans M, Hartford
- Community awareness of postpartum depression. JOGNN – J Obstet Gynecol Neonatal Nurs. 2009;38(2):121–33.
- Jones CJ, Creedy DK, Gamble JA. Australian midwives’ awareness and management of antenatal and postpartum depression. Women and Birth. 2012;25(1):23–8.
- Highet NJ, Gemmill AW, Milgrom Depression in the perinatal period: Awareness, attitudes and knowledge in the Australian population. Aust N Z J Psychiatry. 2011;45(3):223–31.
- Wyatt S, Ostbye T, De Silva V, Lakmali P, Long Predictors and occurrence of antenatal depressive symptoms in Galle, Sri Lanka: a mixed-methods cross-sectional study. BMC Pregnancy Childbirth [Internet]. 2021;21(1):1–13. Available from: https://doi.org/10.1186/s12884-021-04239-w
- Frontier TN, Development The Next Frontier : Human Development and the Anthropocene Sri Lanka. 2021;1–7.