Medical Journal
Published by
Faculty of Medical Sciences,
University of Sri Jayewardenepura,
Nugegoda,
Sri Lanka.
Original Articles
Language barriers in Medical Education: Perceived challenges of English Medium Learning experienced by first year medical undergraduates in Sri Lanka
Abeysinghe CC1, Allana AR1, Anuththara GS1, Atapattu VV1, Dodangoda AI1, De Silva AH2, Goonewardena CSE3
1Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
2Department of Family Medicine, Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
3Department of Community Medicine, Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
Abstract
Background: English medium has been the standard of medical education for several decades in Sri Lanka. Medical students from non-English speaking backgrounds face multiple challenges in English medium learning (EML), which can hinder their academic performance.
Objectives: To describe the perceived English proficiency and language challenges among first year medical undergraduates and to determine the factors associated with EML challenges.
Methods: A descriptive cross-sectional study was conducted among 169 first-year medical students at the Faculty of Medical Sciences, University of Sri Jayewardenepura, using convenience sampling. Data collected via an online self-administered questionnaire and secondary data obtained from English orientation marks were analysed using SPSS-25.
Results: The mean age of participants was 21.53 years (SD = 0.9). The majority (64.5%, n=109) were female, and 87% (n=147) were Sinhalese. Most (60.4%, n=102) had an A grade pass in General English. Most had satisfactory scores in both pre-test [n=147 (87%)] and Post-test [n=132 (78.1%)] assessments during the orientation program. However, speaking was perceived as the most challenging skill, communicating ideas fluently (62%, n=105), presentations (65.1%, n=110) and speaking to lecturers in English (65.1%, n=110). Additionally, students with higher levels of anxiety (45.6%) and lower confidence (43.5%) faced greater challenges (p < 0.05). Many students reported that language related challenges affected their academic performance (75.1%, n=127), particularly in anatomy (81.7%, n=147).
Conclusion: These findings highlight the gap in English speaking skills, emphasising the need for focused language support programs to assist students in building up their confidence and communication skills, particularly in the early stages of medical education.
Keywords: English Medium Learning, Challenges, Medical undergraduates
Introduction
English Medium Learning (EML) has been the norm for medical education in Sri Lanka for several decades, like most other countries. Being a non-native English-speaking country, a significant proportion of medical undergraduates who have completed their primary and secondary school education in Sinhala or Tamil enroll in university with limited proficiency in the English language. The sudden change of medium of learning to English becomes a barrier for most of the students.[1] This transition presents particular challenges in learning medical knowledge, skills, and communication, which could potentially harm their well-being and academic achievements. The English language is not only crucial as a medium of study for medical students but also serves a vital role in pursuing their future careers.[2]
Medical students frequently struggle to comprehend complex medical topics and terminology when they are delivered in English. Medical books, articles and research reports use technical terms of medicine in English.[3] As a result, students with limited English proficiency may experience difficulty in grasping the essence of the subject content, consequently leading to reduced comprehension and academic performance. A study conducted among medical students at the University of Jaffna revealed that a significant proportion of students reported having trouble understanding English-medium course materials.[4] Many of them attempted to translate phrases into their native tongue to enhance their comprehension. International medical students in China reported that their learning experiences were hindered by their lecturers’ poor English communication and accents.[5] Similarly, the medical undergraduates at a University in Saudi Arabia stated that they needed more English for Medical Purposes (EMP) classes to help them become more proficient readers and speakers.[6]
The linguistic barrier impacts exams, since students believe they would perform better if tests were given in their native tongue. According to a study [7], more than half of University of Peradeniya medical students thought that speaking Sinhala during clinical exams would help them communicate more clearly.
Many studies have been conducted to identify such linguistic challenges, mainly in Asian countries. Although some of these studies were conducted in various faculties in several universities in Sri Lanka, less attention has been directed to such challenges faced by medical undergraduates and their associated factors in the Sri Lankan context.
The main aims of this study were to explore the common challenging English language skills among students and the challenging components in their academic courses, and to determine the factors associated with these challenges.
Methodology
A descriptive cross-sectional study was conducted among first-year medical students of the 2019/2020 batch at the Faculty of Medical Sciences in the University of Sri Jayewardenepura. Convenience sampling was used to conduct the study.
Data was collected by a structured and pretested online self-administered questionnaire. The link to the questionnaire was sent to the batch representatives of the 2019/2020 batch, and they were asked to share it among the batchmates. Participation was voluntary, and informed consent was obtained from the participants. To preserve the anonymity of the participants, data was collected without their names. Participants were informed about the privacy and confidentiality of collected data. Ethical clearance was obtained from the Ethics Review Committee of the Faculty of Medical Sciences, University of Sri Jayewardenepura (REC number – CM/02/21).
Likert scales were used to assess challenges, coping strategies and associated factors (such as level of anxiety, confidence). 10 items for the questionnaire were adopted from Evans and Morrison’s (2011) questionnaire on English medium instructions (EMI) linguistic challenges. Secondary data of pre- and post-orientation English marks were collected from the Language and Communication Skills Unit of the Faculty of Medical Sciences, University of Sri Jayewardenepura, with permission of the Dean and Head of Examination Unit. A pretest was performed to assess the clarity and identify shortcomings in the questionnaire.
A total of 169 questionnaires were analysed using SPSS software version 25. Associations were assessed using Chi chi-square test. Statistical significance was taken as p< 0.05.
Results
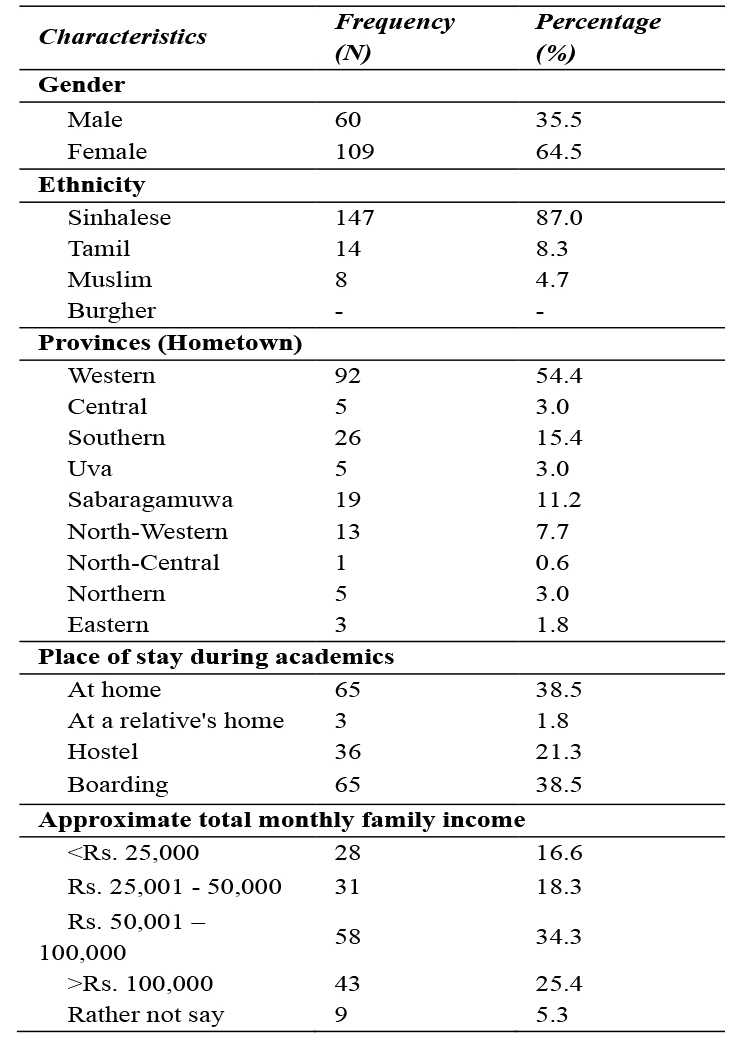
A total of 169 first-year medical undergraduates participated in this study, of whom the majority were females [n=109 (64.5%)]. Their mean age was 21.53 years (SD=0.9), ranging from 20 to 24 years. Most of the study participants were Sinhalese [n=147 (87%)] and from Western province [n=92 (54.4%)]. Almost a quarter (25.4%) of the participants had an approximate total family income of more than Rs. 100,000. The majority of the participants had completed their secondary education at government schools [n=149 (88.2%)], and most had entered university by the second attempt of A/L [n=79 (46.7%)]. (Table 1)
Table 1: Frequency distribution of Sociodemographic and socio-economic characteristics of the study participants (n=169)
Most participants had completed their A/Ls in Sinhala medium [n=134 (79.3%)], while only 24 participants (14.2%) had studied in English medium. The majority had A passes for General English language in both O/L [n=146 (86.4%)] and A/L [n=102 (60.4%)] examinations.
Among the English-related events during schooling, most had participated in writing events [n=118 (69.8%)]; however, participation in other events was poor (<50%), such as drama, speaking, singing and debating.
Nearly half of the study participants [n=84 (49.7%)] had completed an English course/ diploma before university admission. The results of English examinations held during the orientation programme revealed that most students had satisfactory marks for the English Orientation Pre-test [n=147 (87%)] and Post-test [n=132 (78.1%)]. (Figure 1)
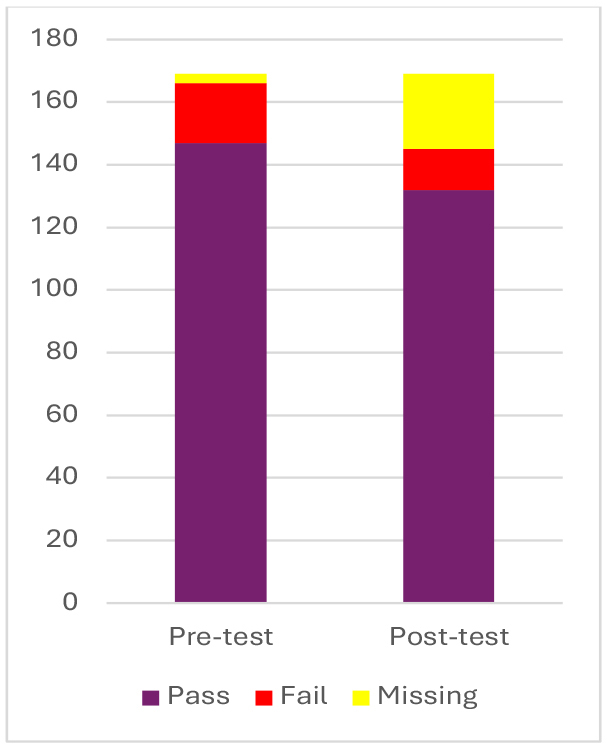
Figure 1: Distribution of pre- — and post-test English orientation marks of the study participants
The common sources used by the study participants to acquire English knowledge were via Internet (94.1%), watching movies (89.9%), TV series (71.6%), reading English books (84.6%), listening to English music (72.2%), whereas listening to English news (41.4%), reading English newspapers (38.5%), and private tuition classes (44.4%) were the less commonly used methods.
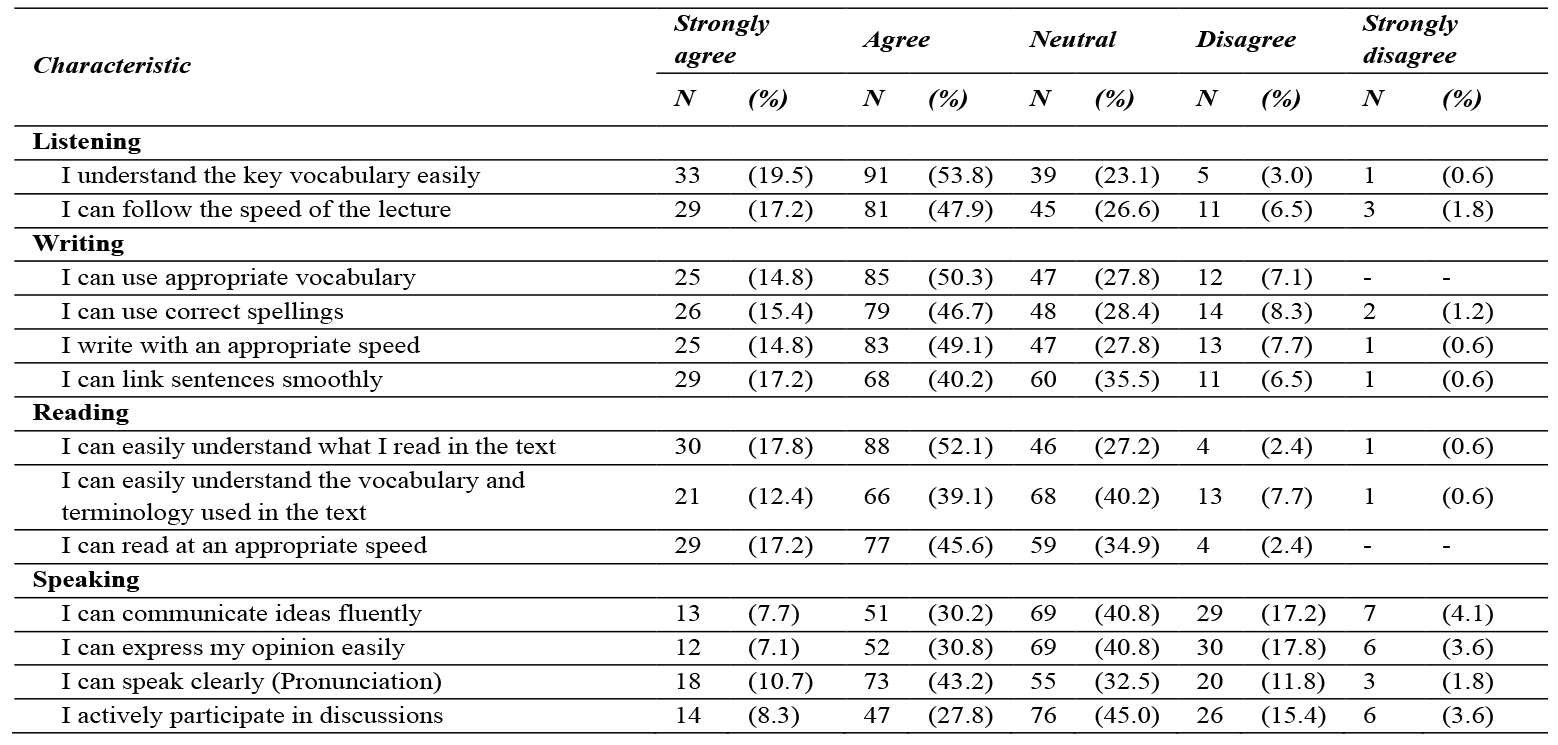
Undergraduate medical students in the first year faced several challenges in English-medium learning. Concerning listening skills, the majority of the study participants agreed that they can understand the key vocabulary easily (53.8%) and follow the lecture speed (47.9%) appropriately. Concerning writing skills, the majority of the participants were able to use appropriate vocabulary (50.3%), correct spellings (46.7%) and also write with an appropriate speed (49.1%). They were also able to link sentences smoothly (40.2%). Concerning reading skills, the majority were able to understand the text (52.1%) and read at an appropriate speed (45.6%), but understanding vocabulary and terminology (40.2%) was somewhat challenging. Speaking was the most challenging skill for most of the participants; they were not able to communicate ideas fluently and express their opinions (62%) (Table 2).
Table 2: Frequency distribution of challenges faced with English medium learning by study Participants
For most of the study participants, facing exams (62.8%), tutorials and SGDs (58.5%), presentations (65.1%) and speaking to lecturers in English (65.1%) were fairly challenging.
The most difficult academic subject was revealed as anatomy (81.7%). The majority of the study participants had difficulties in understanding the lectures occasionally (69.2%). They faced difficulties in understanding the way the lecture was delivered (51.6%). Most of the study participants stated that challenges in English language skills affect their academic performance (75.1%). (Table 3).
Table 3: Frequency distribution of the challenges faced during various occasions among study participants

About half of the study participants were satisfied with the English knowledge gained during the orientation program (50.9%), while a considerable number of participants were not sure whether it was helpful or not (43.8%). Most of the study participants were either not using (54.4%) or occasionally using (29.6%) the University English language support unit to improve their English knowledge.
The level of anxiety and the level of confidence in English medium learning among study participants were assessed using Likert scales. A considerable number of participants had some degree of anxiety (scale -2) about English medium learning (44.4%), while 5.9% had severe anxiety (scale – 4). Additionally, 43.2% were somewhat confident about English medium learning (scale – 2), while only 8.3% were highly confident (scale – 4). (Table 4).
Table 4: Frequency distribution of the level of anxiety and confidence in English medium Learning
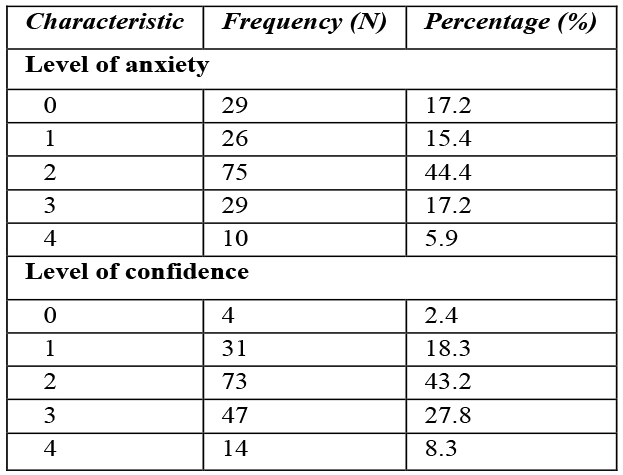
*The level of anxiety was assessed using a Likert scale ranging from 0- no anxiety to 4- severe anxiety.
*The level of confidence was assessed using a Likert scale ranging from 0- no confidence to 4-highly confident
Associations of various factors with challenges in EML revealed several statistically significant findings. It was observed that study participants who had a low level of language anxiety had good knowledge of the English language when compared to those with high language anxiety (82% vs 64%).
This observed difference was statistically significant (p <0.05). But there was no statistically significant difference between the level of confidence with knowledge of the English language (p > 0.05). A statistically significant difference was observed with A/L English results and challenges in EML (p<0.05). Participants with good results in A/L General English (23.9%) face fewer challenges in EML than participants with poor results (65.7%). Those who had good participation in English-related events (25.9%) had fewer challenges than participants with poor participation (58.8%). This observed difference was statistically significant (p<0.05).
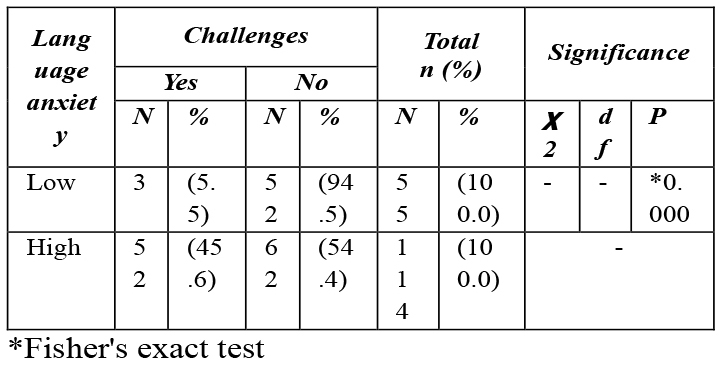
Additionally, there was a statistically significant difference between language anxiety and challenges in EML (p<0.05). Participants with high language-related anxiety had more challenges in EML (45.6%) compared to participants with low anxiety (5.5%) (Table 5). In contrast, a statistically significant difference in the level of confidence and challenges in EML (p<0.05), where participants with a low level of confidence (43.5%) faced more challenges in EML than participants with a high level of confidence (13.1%).
Table 5: Association between language anxiety and challenges in English medium learning among study participants
The following are several responses provided by the students to an open-ended question for suggestions to improve their English proficiency. “Schedule English practice sessions among the batch”. “Add more interactive learning sessions during the orientation period without lecture-like sessions”. “If interactive sessions where we can talk freely in English can be held, it would be great as we can improve language, confidence and release stress”. “It is good if they practice speaking”. “Adding a vocabulary list at the end of each lecture note, if necessary, would be great”. “I like our ELA (English Literary Association) club, I hope there will be dramas and other extra opportunities for us to participate”. “The orientation English program was great. As I’m interested in the language, I’d like it if the program were continued as a short lesson a week or something. As we don’t get professional help for learning English anymore.”
Discussion
This study highlights the challenges faced by first-year medical undergraduates studying in English medium, their coping strategies, and the factors associated with challenges in EML. The results reveal that many students still struggle to adjust to EML in medical faculty, especially when it comes to speaking and comprehending complex material, even though they received relatively high grades in English language at the O/L and A/L levels.
Speaking skills were found to be among the most challenging, with more than 60% of students stating that they had trouble articulating their thoughts and speaking clearly. This result aligns with research conducted in other Asian contexts. Similar difficulties speaking and comprehending spoken lectures were encountered by Saudi Arabian medical students, highlighting the necessity of focused assistance in oral language development.[9] Due to linguistic and cultural limitations, foreign medical students in China reported having trouble understanding what they were hearing and communicating academically.[5]
Many of the students still had trouble understanding academic vocabulary and specialized medical terminology, although more than half of them could follow the pace of lectures and understand ordinary reading material. This suggests that both listening and reading skills are significantly challenged. These results are consistent with previous studies that demonstrated that discipline specific language mastery is still a persistent challenge in English Medium Instruction (EMI) settings, even though receptive skills like reading and listening tend to improve progressively.[10] The complexity of subject-specific language is a fundamental barrier in EML contexts, aligning with the fact that the vast majority of students (81.7%) found anatomy to be especially challenging.
Notably, students who participated actively in English-related school activities and had higher A/L English language results reported fewer EML challenges. This reinforces the idea that early and varied exposure to the English language- particularly through interactive or verbal elements-improves preparedness for EML contexts. Similar findings were reported in Thailand and Malaysia, where pre-university language background significantly affected medical students’ confidence and adaptation in EMI programs.[11], [12]
Another critical contributary factor towards challenges in EML was language anxiety. An inverse relationship was observed between language related anxiety and language performance. Students with low anxiety experienced comparatively fewer EML challenges than those with high language related anxiety, thus impacting their language related academic performance. This highlights the importance of psychological preparedness alongside linguistic training.[13] Furthermore, confidence levels also showed a statistically significant relationship with performance; students with lower confidence were more likely to encounter difficulties, indicating a potential area for help through structured communication practice and peer interaction.
Conclusions
EML continues to pose substantial academic and psychological challenges for medical undergraduates. Improving early language exposure, promoting active coping methods, and strengthening institutional support-particularly for speaking and terminology comprehension-are critical. These findings highlight the necessity for medical schools to incorporate systematic English support into the curriculum in order to enhance both language and academic competence.
Recommendations
At the university level, English orientation programs should place greater emphasis on improving students’ grammar and speaking abilities. Additionally, the English language support units within faculties should offer extended assistance, particularly to students who demonstrate weaker proficiency. To further aid learning, universities should implement systems that allow students to clarify grammar-related doubts through accessible online platforms such as email, blogs, or discussion forums. Peer support groups, English classes can also be established through the Language support unit for students who are hoping to improve their language skills.
Acknowledgement
We sincerely express our gratitude to all the participants who provided their support by participating in our study. We would also like to thank the Department of Community Medicine, Faculty of Medical Sciences, University of Sri Jayewardenepura, for the extensive support provided.
Abbreviations
AL – Advanced Level
EML – English Medium Learning
OL – Ordinary Level
Ethics approval and consent to participate:
Consent and Ethics approval from the research ethics committee of the Faculty of Medical Sciences, University of Sri Jayewardenepura. (Rec no – CM/02/21) – Annexed
Consent for publication: Consent implied
Availability of data and material:
The data sets used/or analysed during the current study are available from the corresponding author upon request.
Competing interests: No financial or non-financial competing interests
Funding: None
Author’s contribution
CCA, ARA, GSA, VVA and AID contributed to the literature search, methodology, acquisition of data, analysis and interpretation of data and drafting the manuscript. The conceptualisation of the study was done by CSEG and AHDS, who were the overall supervisors. All authors proofread the final version of the manuscript.
References
- Seneviratne T, Perera H, Wijesinghe S, Fernando S. Sinhala as the medium of instruction in medical education: Perception of medical students in Sri Lanka. Asia Pac Scholar. 2019;4(3):48-56. doi:10.29060/taps.2019-4-3/oa2090
- Niazi MM. English for medical purposes: A case of English for Specific Purposes. Islamabad, Pakistan: National University of Modern Languages; 2012.
- Budianto L. Students’ needs in learning English in the medical faculty of Muhammadiyah University at Malang. J Ilmu Pendidik. 2004;11(3):\[page numbers missing]. Available from: [https://www.researchgate.net/publication](https://www.researchgate.net/publication)
- Weerasinghe RHM, Lakmali JMD, De Silva BHKG, Kumar R, Sathiadas MG. Burnout syndrome, associated factors and coping strategies of Jaffna medical students. Jaffna Med J. 2020;32(1):12-17. doi:10.4038/jmj.v32i1.87
- Li L, Zhang Z, Wang X, Li Y, Li Y, Li X. International medical students’ perspectives on factors affecting their academic success in China: A qualitative study. BMC Med Educ. 2022;\[volume and page numbers pending].
- Javid Z. EMP needs of medical undergraduates in a Saudi context. arXiv. 2014. Available from: [https://arxiv.org/](https://arxiv.org/)
- Perera H, Wijesinghe S, Fernando S. Sinhala as the medium of instruction in medical education: Perception of medical students in Sri Lanka. Asia Pac Scholar. 2020. Available from: [https://medicine.nus.edu.sg/taps/issues/Sinhala -as-the-medium-of-instruction-in-medical education – perception-of-medical-students-insrilanka/] (https://medicine.nus.edu.sg/taps/issues/sinhala-as-the-medium-of-instruction-inmedical-education-perception-of-medicalstudents-in-sri-lanka/)
- Evans S, Morrison B. Meeting the challenges of English-medium higher education: The first-year experience in Hong Kong. Engl Specif Purp. 2011;30(3):198-208.doi:10.1016/j.esp.2011.01.001
- Alanazi K, Curle S. Challenges experienced by students studying medicine through English medium instruction. Front Educ. 2024;9:\[page numbers pending]. doi:10.3389/feduc.2024.1364860
- Yang J, Li X, Zhang Z, Li Y, Wang X, Li Y. Challenges and adaptations in implementing an English-medium medical program: A case study in China. BMC Med Educ. 2019;19:15. doi:10.1186/s12909-018-1452-3
- Yusoff MSB. A multi-ethnic study of stress levels among first-year medical students in Malaysia. Malays J Med Sci. 2011;18(1):21-27.
- Rujirojindakul P, et al. Stress and coping strategies among medical students in Thailand. Siriraj Med J. 2020;72(2):129-135.
- Wu L, et al. Understanding Singaporean medical students’ stress and coping. Singapore Med J. 2018;59(4):172-176.