Medical Journal
Published by
Faculty of Medical Sciences,
University of Sri Jayewardenepura,
Nugegoda,
Sri Lanka.
Leading Article
Student Perceptions and Preparedness: Are Medical Students Ready for AI in Resource-poor Countries?
Indrakumar J
Chair Professor of Medicine, Faculty of Medical Sciences, University of Sri Jayewardenepura.
indrak2004@gmail.com
Abstract
The integration of artificial intelligence (AI) into medical education is increasingly recognised as essential for the advancement of healthcare systems globally. Medical schools in resource-poor countries, such as Sri Lanka, encounter significant challenges when incorporating AI into their curricula. This study explores medical students’ perceptions of AI in healthcare and identifies barriers to its integration into medical education in resource-limited settings. A review of existing evidence was conducted, focusing on Southeast Asian medical students’ attitudes toward AI and the current state of AI education in these regions. Medical students in Southeast Asia view AI positively for healthcare advancement but lack knowledge and preparedness to use AI tools. Medical curricula do not adequately address AI education, leaving students unprepared for healthcare demands. Barriers include limited infrastructure, financial constraints, faculty unpreparedness, and ethical concerns. To address these challenges, AI training programs should utilize open resources and prioritise faculty development. Successful AI integration will require collaboration among medical schools, healthcare institutions, and technology companies. By focusing on context specific AI education and addressing challenges in resource-limited countries, medical schools can prepare physicians to utilise AI effectively. Collaborative efforts are needed to align medical education with healthcare needs.
Keywords: Artificial Intelligence, Medical Education, Resource-poor Countries, Student Perceptions, Preparedness, Curriculum Integration, Healthcare Challenges
Introduction
Integrating Artificial Intelligence (AI) into medical education is becoming inevitable for the development of healthcare, as it can greatly improve how future doctors are trained. Large language model (LLM) AI tools, ChatGPT, tools for reading medical images, clinical decision support systems, and telemedicine are already changing healthcare in developed countries [1]. These developments improve the accuracy of diagnosis and treatment and make health services more effective. There is growing agreement that AI should be incorporated into medical education [2]. However, adding AI to medical curricula in countries with limited resources, such as Sri Lanka, is challenging because there is limited technology, a shortage of healthcare workers, and funding constraints. These issues make the implementation of AI in medical education difficult.
This paper aims to examine how medical students in resource-poor countries, especially in Southeast Asia, feel about using AI in their education and how ready they are for it. It provides an overview of AI education in medical schools by synthesizing peer-reviewed studies. Furthermore, this paper identifies regional trends and highlights the challenges and opportunities of integrating AI into medical curricula. This paper aims to help create AI training programs that fit local needs. This will ensure that future doctors are ready for changes in healthcare technology.
Our country faces healthcare challenges owing to limited resources, inadequate infrastructure, healthcare worker shortages, and financial constraints. The integration of AI into healthcare systems offers cost-effective solutions, remote access, and improved worker efficiency. As technology transforms medical education, understanding how students perceive and prepare for AI is crucial to its ethical integration into the curriculum.
This article examines peer-reviewed studies on medical students’ perceptions and preparedness for AI integration into medical education, focusing mainly on resource-poor countries in Southeast Asia. Thereafter, it discusses the problems faced by countries that have limited resources. By identifying research gaps and regional trends, this study attempts to guide the effective integration of AI into medical education, overcoming the challenges faced in our country, so that future doctors are properly trained to work with AI. These findings can help to create training programs for future doctors. These programs will teach them to work with AI systems and meet the country’s future healthcare needs.
Global Context of AI in Medical Education
The integration of AI into the medical curricula is a challenge. AI can significantly improve medical education. Top universities, such as Harvard Medical School, are at the forefront of using innovative methods to teach AI. These initiatives will help future doctors learn important skills and improve healthcare delivery. However, we need to be mindful of the ethical, legal, and practical issues associated with using AI. In this way, we can maximise the benefits and minimise potential problems.
Recent studies have shown that medical students recognise AI’s capability to make health care much more efficient. They feel the need to be exposed to AI early in their curriculum. An international multicentre cross-sectional study to assess AI knowledge, attitudes, and education among medical, dentistry, and veterinary students from 192 faculties in 48 developed countries found that approximately 67.6% of students generally perceived the integration of artificial intelligence (AI) in healthcare positively. Furthermore, 76.1% expressed a desire for more AI-related content to be incorporated into their curriculum. However, 75.3% acknowledged that they had limited knowledge of AI, and 76.3% reported the absence of formal AI courses. Additionally, 57.9% felt unprepared to apply AI in their prospective medical careers [3]. Subgroup analyses revealed regional differences in perceptions, although these differences were relatively small. These findings highlight a significant global gap between the increasing integration of AI in healthcare and educational preparation.
Challenges Faced by Resource-Poor Countries
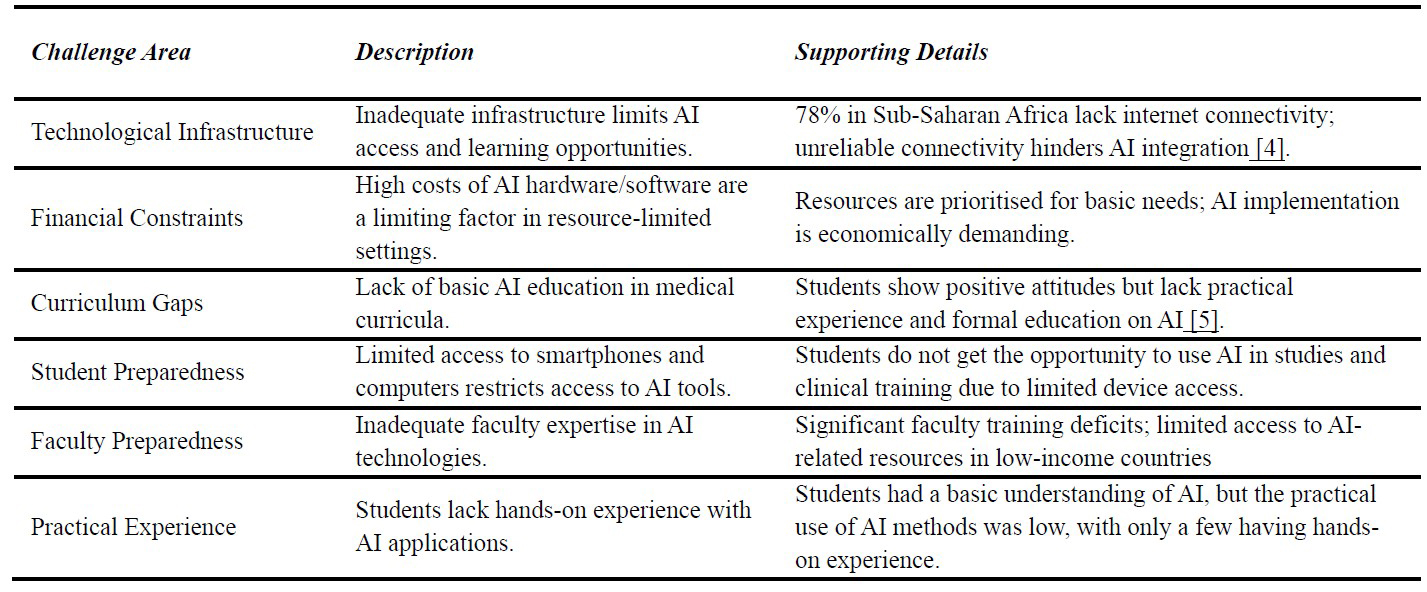
Introduction of AI to the medical curriculum faces special problems in countries with fewer resources compared to richer countries. Table 1 shows the main differences between these countries when it comes to AI in medical education.
Table 1: Challenges in integrating Artificial Intelligence into Medical education
Student Perceptions of AI in Medical Education in Southeast Asia Medical students worldwide acknowledge the increasing significance of AI in health care. Therefore, there is a strong need for AI education in medical schools. This finding demonstrates the importance of adding AI to medical training.
Studies from Vietnam have shown that most undergraduate medical students have little prior understanding of the role of AIs in healthcare. However, the majority expressed positive views, showing an interest in learning the fundamentals and applications of AI in medicine [6]. Likewise, in Nepal, studies show that medical students have limited AI understanding but recognise the potential impact on their careers and are willing to learn. They are uncertain about its implications for the healthcare system due to a lack of AI education in the current curriculum [7].
In both Malaysia and Bangladesh, a large number of medical students believe that AI will have a significant impact on medicine and improve medical practice. Most recognise AI’s importance for their future careers and advocate for its formal integration into medical curricula [8,9]. Medical students in Thailand have shown a limited understanding of AI and its applications in healthcare, but they are strongly supportive of integrating AI training into their medical education [10]. In Indonesia, medical students typically show neutral to positive attitudes toward their preparedness, understanding, and views on AI.[11].
The evidence presented above indicates that medical students across Vietnam, Nepal, Bangladesh, Malaysia, Thailand, and Indonesia share a common pattern.
- Most students have limited knowledge of AI and its applications in healthcare.
- Most express positive attitudes and are very much interested in learning AI basics.
- They recognised the inevitable use of AI in their future careers and understood its potential impact.
- There is strong support for incorporating AI training into medical curricula.
- These findings show that students do not know much about AI, but want to learn it. The question is whether medical schools are ready to teach AI. Adding AI to the curriculum could help students prepare for changes in health care technology.
Student concerns regarding the integration of AI in medical curricula
While they express enthusiasm, they also have apprehensions and concerns regarding the integration of artificial intelligence into medical education and their professional roles.
- Fear of losing jobs: Many students worry that AI might take over their doctors’ jobs. For example, the fear of AI taking over radiology has made many medical students avoid choosing radiology as their career.
- Dehumanisation due to AI integration: Concerns exist regarding medicine’s dehumanisation as AI enters healthcare. A Nigerian survey showed that 70.6% of medical students feared that AI could reduce their personal patient care [12].
- Ethical and societal challenges: People are worried about data privacy, bias in algorithms, transparency, accountability when there is an error, and how it affects the doctor-patient relationship.
- Scepticism about AI’s abilities: Some students express scepticism regarding the capability of artificial intelligence to effectively manage tasks that inherently require emotional intelligence, empathy, personal interaction, and psychological counselling. [13]
- Job openings in the medical field lower the demand. AI systems can analyse images and perform routine tests. This might mean fewer doctors are needed in fields like radiology.
- Speciality choices affected: AI’s influence on job markets affects medical students’ speciality choices. They avoided radiology owing to AI. Most researchers believe that AI will revolutionise radiology [14].
- Future workforce implications: Students are concerned about the impact of AI on medicine. For instance, they wonder, if AI handles most of the tasks, what will be left for me to do?
Student Preparedness for AI in Healthcare in Southeast Asia
Although students in our region express positive attitudes towards artificial intelligence (AI), they are not yet adequately prepared to use it effectively. Several studies suggest that medical students in Southeast Asia generally possess limited knowledge of AI and its applications in the healthcare sector. [15].
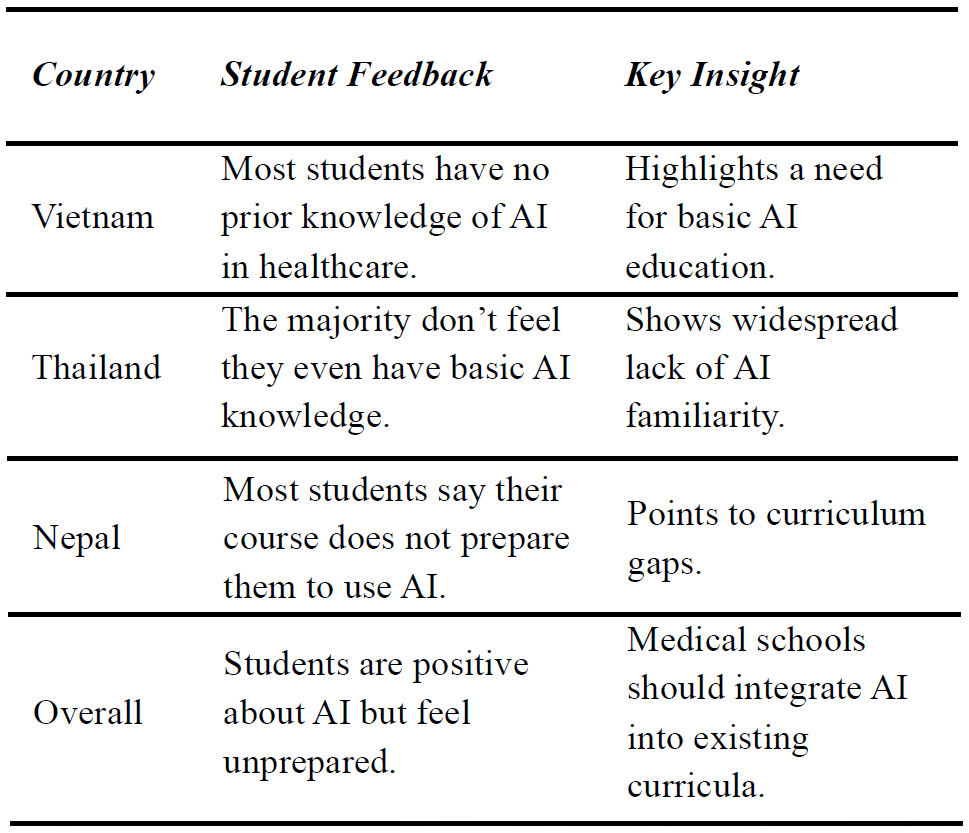
In Vietnam, the majority of medical undergraduates reported a complete lack of prior knowledge regarding AI’s role in healthcare and how to use AI tools in healthcare [6]. Likewise, in Thailand, most medical students do not think that they have basic knowledge about AI [10]. In Nepal, most students expressed that the current medical course did not teach them the necessary skills to use AI in their field [7]. This difference between students’ positive attitude toward AI and not feeling prepared shows that medical schools in these regions need to incorporate AI education into what they already teach. Table 2 highlights the significant gaps in AI knowledge and preparedness among medical students in Southeast Asia.
Research shows that tools such as the Medical Artificial Intelligence Readiness Scale can assess medical students’ readiness for AI in healthcare [11]. These tools not only provide a clear picture of student preparedness but also help educators monitor progress and design more effective AI training programs.
Table 2: AI Knowledge and AI Preparedness Among Medical Students in Southeast Asia
Challenges and Barriers in Resource-Poor Settings
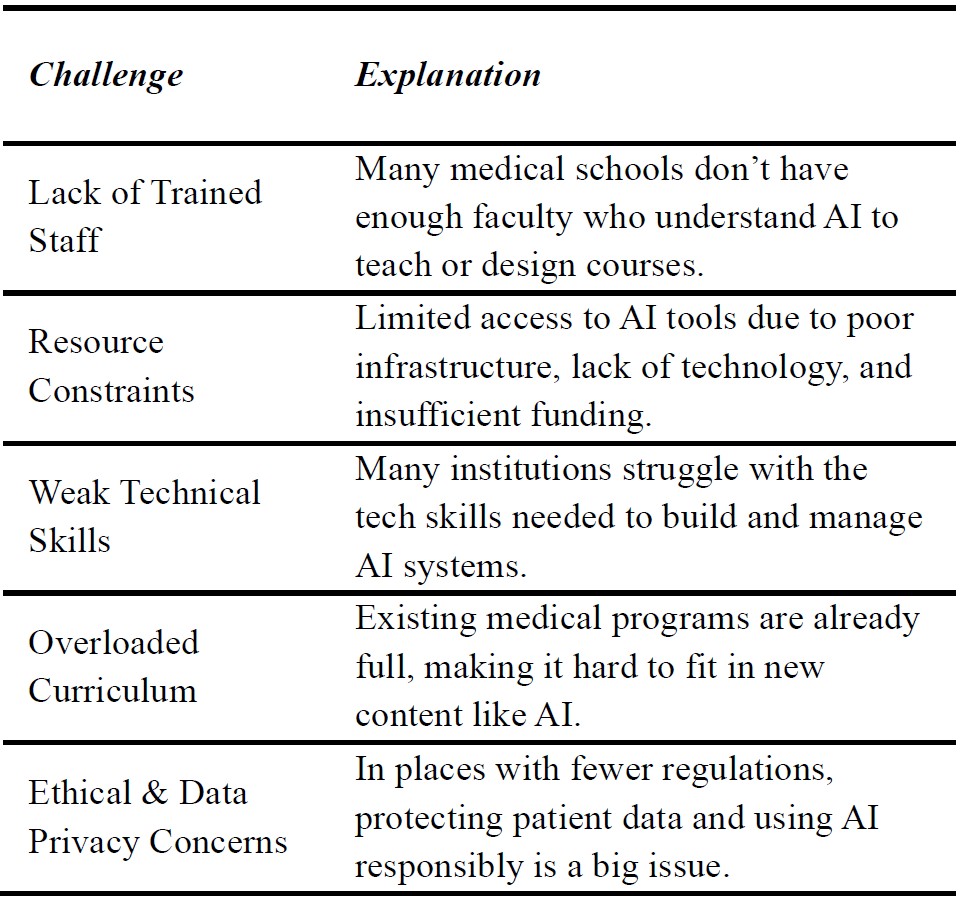
The incorporation of Artificial Intelligence (AI) into medical education in Sri Lankan medical schools is a major challenge. One major problem is the significant shortage of staff trained in AI, which makes it extremely difficult to create and implement relevant courses [16]. It is difficult to create modern AI training environments because there is not enough access to technology, stable internet access, and funding. These problems are further complicated by deficiencies in technical skills and the basic infrastructure to develop and maintain AI systems. Concerns regarding ethics and data privacy have exacerbated these issues. When educational and regulatory authorities do not provide clear guidance, they confuse, and institutions do not know what to do. Medical courses are already full; therefore, adding AI would require a large restructuring process. With all of these major obstacles, the need for AI integration is growing, as AI is significantly changing and rapidly impacting healthcare, and our future doctors need to be well prepared.
Table 3: Challenges to integrating AI in medical education in Southeast Asia:
Future Directions and Recommendations
To include AI in medical education, we should first assess the perceptions and preparedness of medical students regarding AI. We can do this using surveys, interviews, and group discussions, which will help us understand their views and readiness for AI.
We need to develop and evaluate AI training programs tailored to local contexts to ensure they are relevant. Starting AI lessons early in medical school helps students think critically and find complex information.[17]. It is also crucial that medical schools establish clear ethical guidelines for AI use in education and healthcare.
Therefore, continuous evaluation and improvement of AI training programs are necessary. Regular evaluation of their effectiveness allows us to refine the curriculum and enhance student learning. To ensure continued relevance and effectiveness, AI education must adapt its curriculum in response to evolving changes in healthcare AI. Furthermore, AI should be incorporated into the current medical curriculum, instead of being taught as a separate subject [18].
The curriculum should include flexible and affordable modular programmes. Programs should use free tools and rely less on technology. Policies and funding are needed to enhance digital resources and train educators, as a lack of AI-skilled teachers makes integration difficult. Teachers should participate in workshops and collaborate with AI specialists by utilising resources to integrate AI into their teaching methods. [19] To overcome financial barriers, free online resources such as YouTube videos, open-access courses, and AI simulations should be encouraged, making AI training more accessible and affordable for medical students.
A key challenge for our institutions is the limited technology infrastructure and poor internet access. This can be resolved by developing offline learning materials, mobile education applications, and establishing community tech hubs equipped with computers and AI software. Partnerships with technology companies and non-governmental organisations (NGOs) could provide valuable support in bridging these gaps.
As AI continues to grow in medical education and healthcare, establishing ethical guidelines and transparency is crucial. Institutions must ensure that AI is used ethically and fairly. Training programs should prepare healthcare workers to address ethical challenges as AI becomes more prevalent in practice.
Thus, we should explore how artificial intelligence can support health priorities in resource poor regions. AI tools can enhance surveillance and control of infectious diseases, improve maternal health through antenatal data analysis and remote monitoring, and support the management of chronic non-communicable diseases in low- and middle-income countries like ours. AI-driven tools for risk prediction, treatment optimisation, and self management could contribute to better disease prevention and care in resource-limited regions. Prioritising AI tools for local health needs will ensure a fair distribution of benefits and improve access for underserved populations.
AI technology can improve health care in hard-to-reach areas by enabling doctors to treat distant patients. Through AI, providers can monitor health and create personalised treatment plans, thus benefiting those with limited access to medical care. AI-based telehealth reduces healthcare inequalities, improves outcomes, and saves costs [20].
The collaboration between medical schools, healthcare institutions, policymakers, and technology companies is crucial for the integration of artificial intelligence into medical education. By sharing resources and engaging in cross-national cooperation, we can effectively prepare future physicians for AI-enhanced healthcare environments.
Conclusion
In conclusion, using artificial intelligence (AI) in medical education, especially in regions with limited resources, can significantly improve healthcare. It is necessary to teach medical students AI skills and knowledge to keep up with the changes in medicine. There is a strong need to include AI in the curriculum, offer accessible training resources, and solve infrastructure issues so that all medical students can learn AI equally. The focus should be on creating simple, flexible programs that do not depend heavily on technology and instead use free tools. It is also crucial to address the lack of teachers with AI skills by offering training workshops, collaborating with AI experts, and providing support. Using free online resources, tools, and platforms, we can overcome financial and technological barriers, making AI training more accessible and affordable.
References
- Maleki Varnosfaderani S, Forouzanfar M. The role of AI in hospitals and clinics: transforming healthcare in the 21st century. Bioengineering. 2024 Mar 29;11(4):337.
- Suresh N, Rajprasath R, Elantamilan D, Arghya D. Artificial intelligence revolutionising the field of medical education. Cureus. 2023;15(11): e0.
- Busch F, Hoffmann L, Truhn D, Ortiz-Prado E, Makowski M, Bressem K, Adams L. Medical students’ perceptions towards artificial intelligence in education and practice: a multinational, multicentre cross-sectional study. medRxiv [Preprint]. 2023 Dec 9:2023.12.09.23299744. doi:10.1101/2023.12.09.23299744.
- Wobo KN, Nnamani IO, Alinnor EA, Gabriel- Job N, Paul N. Medical students’ perception of the use of artificial intelligence in medical education. Int J Res Med Sci. 2025 Jan;13(1):82.
- Amin MH, Elmahi MA, Abdelmonim GA, Fadlalmoula GA, Amin JH, Awad MH, Dayyeh NT, Abdalkareem NA, Ahmed EM, Osman HA, Mohamed HA. Knowledge, attitude, and practice of artificial intelligence among medical students in Sudan: a cross-sectional study. Ann Med Surg (Lond). 2024 Jul 1;86(7):3917-23.
- Truong NM, Vo TQ, Tran HT, Nguyen HT, Pham VN. Healthcare students’ knowledge, attitudes, and perspectives toward artificial intelligence in southern Vietnam. Heliyon. 2023 Dec 1;9(12):e21177.
- Jha N, Shankar PR, Al-Betar MA, Mukhia R, Hada K, Palaian S. Undergraduate medical students’ and interns’ knowledge and perception of artificial intelligence in medicine. Adv Med Educ Pract. 2022 Aug 23;13:927-35
- Binte Islam, Aftabi N. Final year BDS student perception of artificial intelligence use in dental practice. J Prev Soc Med. 2024;41(1):50-3. doi:10.3329/jopsom.v41i1.66643.
- Tung AYZ, Dong LW. Malaysian medical students’ attitudes and readiness toward AI (artificial intelligence): a cross-sectional study. J Med Educ Curric Dev. 2023;10:1-7.
- Angkurawaranon S, Inmutto N, Bannangkoon K, Wonghan S, Kham-Ai T, Khumma P, et al. Attitudes and perceptions of Thai medical students regarding artificial intelligence in radiology and medicine. BMC Med Educ. 2024;24:1188.
- Lugito NPH, Cucunawangsih C, Suryadinata N, Kurniawan A, Wijayanto R, Sungono V, et al. Readiness, knowledge, and perception towards artificial intelligence of medical students at Faculty of Medicine, Pelita Harapan University, Indonesia: a cross-sectional study. BMC Med Educ. 2024;24:1044.
- Oluwadiya K, Adeoti A, Agodirin S, Nottidge T, Usman MI, Gali MB, et al. Exploring artificial intelligence in the Nigerian medical educational space: an online cross-sectional study of perceptions, risks and benefits among students and lecturers from ten universities. Niger Postgrad Med J. 2023;30:285-91.
- Mehta N, Harish V, Bilimoria K, Morgado F, Ginsburg S, Law M, Das S. Knowledge of and attitudes on artificial intelligence in healthcare: a provincial survey study of medical students. medRxiv [Preprint]. 2021 Jan 15:2021.01.15.21249862. doi:10.1101/2021.01.15.21249862
- Hassankhani A, Amoukhteh M, Valizadeh P, Jannatdoust P, Sabeghi P, Gholamrezanezhad A. Radiology as a specialty in the era of artificial intelligence: a systematic review and meta-analysis on medical students, radiology trainees, and radiologists. Acad Radiol. 2023;30:306-17.
- Pupic N, Ghaffari-Zadeh A, Hu R, Singla R, Darras K, Karwowska A, et al. An evidence based approach to artificial intelligence education for medical students: a systematic review. PLOS Digit Health. 2023;2:e0000251.
- Grunhut J, Marques O, Wyatt AT. Needs, challenges, and applications of artificial intelligence in medical education curriculum. JMIR Med Educ. 2022;8:e35705.
- Xu Y, Jiang Z, Ting DSW, Kow AWC, Bello F, Car J, et al. Medical education and physician training in the era of artificial intelligence. Singapore Med J. 2024;65:159-65.
- Krive J, Isola M, Chang L, Patel T, Anderson MC, Sreedhar R. Grounded in reality: artificial intelligence in medical education. JAMIA Open. 2023;6:ooad065.
- D’Souza R, Mathew M, Mishra V, Surapaneni KM. Twelve tips for addressing ethical concerns in the implementation of artificial intelligence in medical education. Med Educ Online. 2024;29:2364642.
- Rintyarna BS, Sasmiyanto S, Insantuan OD, Widiawati I, Purwoko RY. Telehealth in remote areas: a new artificial intelligence-based model. Int J Sci Soc. 2023;5:243-50.